
How to get doctors to use your innovation
Subtitle: The inside scoop on what your idea or product needs to scale
By Olivia Geen, MD, MSc, FRCPC
| 15 min read |
It was a classic story. The startup I was working with had come up with an amazing idea that solved an important problem. They were convinced it was going to change the world in a big way. They had built their solution into a great product using their own money and venture capital funding.
The whole team, myself included, felt excited, motivated, and full of hope and possibility.
But nothing happened. No one was rushing to use the solution, to send patients, sign up, and benefit from this great innovation. It had hit the impenetrable wall of healthcare.
This is an issue for both innovators outside the traditional hospital walls (entrepreneurs), like this example, and innovators inside (researchers, service providers, admin, etc). The black box exists for anyone who has ever tried to change or improve anything in healthcare.
The following post will walk you through 5 of the major reasons things fail in healthcare, and what you can do to improve your chances of success. It draws from theories in translational health sciences along with insights from my own real-world experience in healthcare as a doctor, and as an advisor for healthcare startups.
Before we begin, let’s quickly define what innovation is so we’re on the same OG page.
WHAT IS INNOVATION?
The simplest way is to define innovation as anything that’s new. This is often said to include new ideas (“we should prescribe less benzodiazepines in hospital”) or new products (“I developed this app that helps triage patient referrals more quickly”).
I personally think it’s more useful to consider ideas as the “what” we’re going to do that’s new, and the product as the “how” we’re going to actually put that idea into the real, tangible world.
With this definition, you can see that if you have a cool idea, there’s a list of ways that you can try and make it happen (below, not exhaustive). You can also see right off the bat that if your innovation is still just an idea, that’s why it’s not being used. You need to transform it into something, or give it some kind of raft, to get into the real world; out of your head, and into the heads of others. A policy document or guideline doesn’t do anything unless you build it a boat to sail into people’s physical day-to-day world.

Now that we all know what an innovation is (a new, tangible, thing), let’s get to why people might not be using yours.
WHY AREN’T PEOPLE USING MY INNOVATION?
After studying at Oxford and working with several startups in formal and informal roles, there are 5 key patterns that I see in the research and in real-life.
The first 3 reasons actually boil down to one, overarching problem. If your innovation isn’t making it’s way into healthcare… it’s because people don’t want it. It’s really that simple.
At the end of the day, you’ve got to give the people what they want - short of laws and regulations, you can’t force people to do anything (and even then, people find ways around it). There are ways to make people more willing to use your innovation (e.g. incentives), but ultimately, they have to want to say “yes” more than they want to say “no” to your idea. It’s human nature to weigh our decisions, and say yes to the thing that serves our interests the most.

You can then get on with fixing the problem by asking yourself “why don't people want my thing?”. You’ll likely find that the answer relates to one of the following 5 reasons.
5 reasons why your innovation isn’t being used by healthcare providers:
They don’t have the problem your innovation solves
They have other more important problems
Your innovation doesn’t actually solve the problem
They don’t have the bandwidth or resources to use your innovation
They don’t trust your innovation
I’ll explain each of these in more detail, and what you can do to overcome them.

1. THEY DON’T HAVE THE PROBLEM YOUR INNOVATION SOLVES
This is one of the biggest misconceptions about healthcare innovation, particularly when people unfamiliar with entrepreneurship try and get an idea to become a reality. The big mistake is thinking that your problem is everyone’s problem. The classic “pet project” problem. Just because you care, doesn’t mean other people do (sorry!).
For example, one of the reasons why the startup I mentioned wouldn’t spread is that they were trying to get all family doctors to use it. Turns out, not all doctors had the problem we were solving. Only some of them did. For the rest, they didn’t really see the value-add, or value-proposition, as it’s called in the biz.
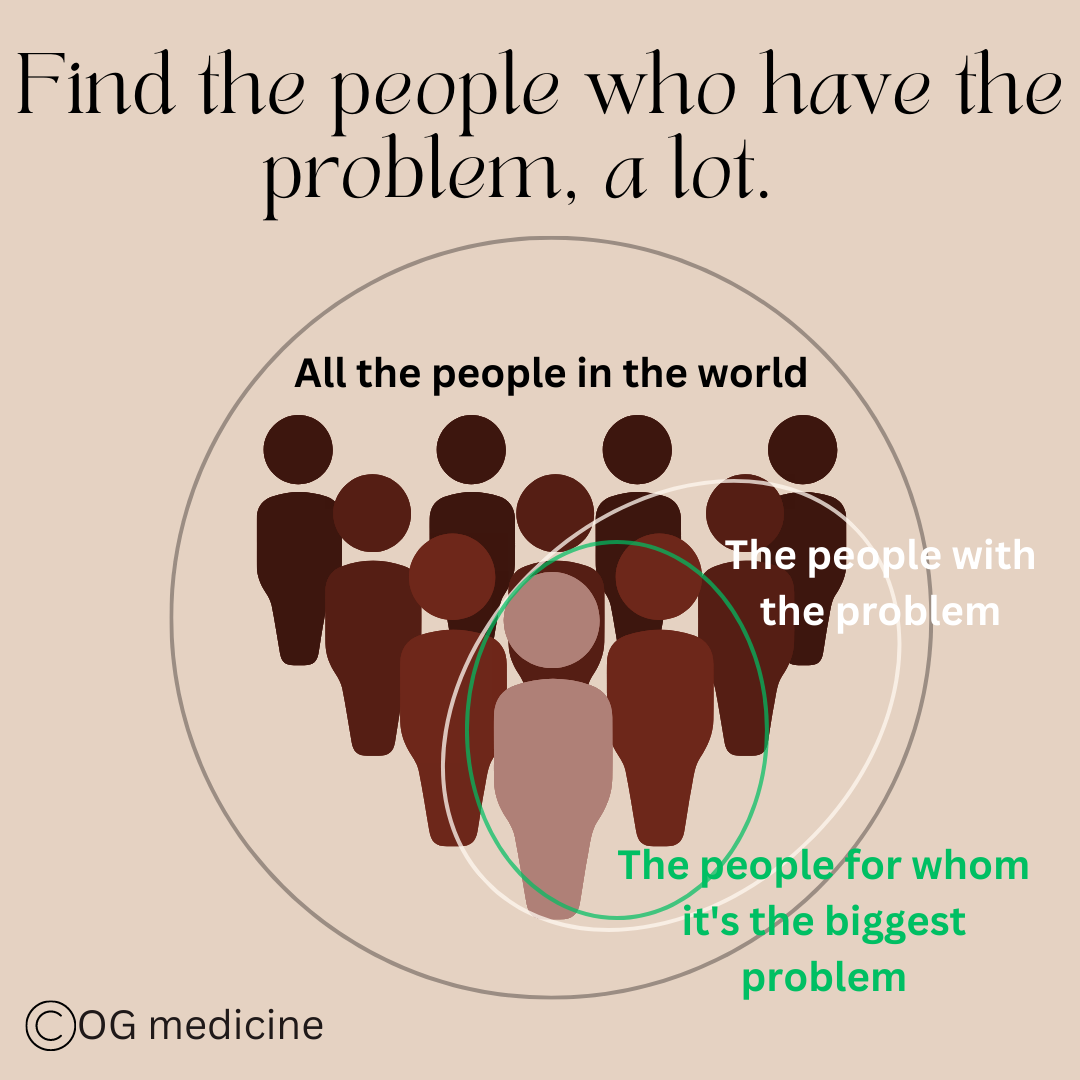
What you want to do is find the people who have your problem, and ignore the rest. This is the concept of target market.

If people don’t have the problem, it’s extremely hard (read: near impossible) to get them to use your product.
It’s important to highlight the difference between not having the problem at all, and not knowing that you have it. For example, a dermatologist does not have the problem of needing a new surgical drill - that’s a problem for the orthopods. You’re never going to convince a dermatologist to use a drill.
On the other hand, in the case of the startup, some doctors did actually have the problem but they didn’t know it, because it was around deprescribing of a particular medication that wasn’t widely done in practice at the time.
Not knowing, or problem-blindness, is a potential market, but it takes a huge amount of effort to overcome when you’re first starting out - you’ll need to launch a big marketing/communication/education campaign to reveal to people that the problem exists for them. Most of us don’t have the funds or time for that.
This means that if you’re not the government or public health, then it’s best to just focus on the people that already know they have your problem, and lump “not knowing” and “not having” together into the group that you won’t be able to reach initially.
Overtime, through diffusion of innovation, it’s possible for your product to spread to the problem-blind as more people see it and realize that they have the problem too. In a future blog we’ll go into diffusion of innovation in more detail, but for now, here’s the original research paper about it.
2. THEY HAVE OTHER MORE IMPORTANT PROBLEMS
This, and #3, are probably the issues that I see most often with early-stage healthcare innovators. I’m just going to say it. Healthcare is a mess. There are problems left, right, and centre.
The two biggest problems driving most of the mess can be summarized as
there are not enough trained people to do the job and
the job is really complicated and hard and it takes a lot of time to do it well.
Or, in other words, we have a capacity issue. That’s it. That’s the biggest problem. Almost everyone who works in healthcare will want you to solve this problem first or at the very least not make this problem worse with your innovation. I see a lot of potential solutions that are great in theory, but they add work for the doctor, nurse, administrator, etc, and we simply do not have the time for that.

Every day in healthcare is packed with work - in the places that need innovation the most, often there just isn’t the time to incorporate something new. That is, unless your innovation can improve efficiency and is easy to use, saving time from the moment healthcare workers start to use it.
What can you do about it?
Explain how your innovation either a) takes work off their plate and/or b) makes the job easier to do
You have to link your innovation to the main big problem of capacity that they are grappling with every day. Otherwise it’s a tough sell for them to invest time in acquiring and integrating a new innovation into their lives.
In the case of the deprescribing startup, we monitored patients for the family doctors using validated tools (like the PHQ-9), which they would otherwise have had to do. This made a clear case of how we were making life easier and taking work off their plate.
2. Make your innovation really easy to use
Don’t make life harder. You’d be surprised how many startups miss this very crucial point, because they see a problem and think “this is terrible! We must do something about this!”. You’re right. It is terrible, and we should. But there are more immediate fish to fry, like doing the basics of day-to-day medical care, and healthcare stops for no one. If your idea makes a jam-packed day harder and longer, healthcare workers will resist, ignore, and eventually throw-out the very well-intentioned thing that you made.
The key to being easy to use is to make it simple. If you can’t make your innovation simple, you’ll need to find ways to offset the trouble of incorporating the innovation into practice. This could mean having hands-on support (like IT people at the ready to trouble-shoot a new technology), incentivizing its use (e.g. money), or removing some other aspect of work while you’re implementing the new innovation (e.g. removing some other admin task that frees up the doctor’s time to try something new).
3. Find people who are unusually invested in your problem
The final option is to find people for whom the problem is number one, despite the background capacity issue. In this example, this meant finding family doctors with patient populations with high mental health needs, and next to no mental health supports. For them, incorporating a new task (recommending the startup to patients) might be worth it, because the alternative is no help at all.
This links back to our first issue, of making sure you target the people with the problem. You can take that one step further and find the very particular smaller group of people who really have your problem, and then slowly scale out from there as you gain traction and figure out the kinks in your plan.
3. YOUR INNOVATION DOESN’T ACTUALLY SOLVE THE PROBLEM
This is another big one. It’s very common to come up with an innovation that you think solves a problem, but it turns out you’re just solving a surface-level piece of the problem. You have to get to the root of the issue to really fix it.
For example, I could observe that patients often don’t show up to my appointments in my geriatric medicine clinic. I could say to myself - “they must be forgetting to come!”. So I decide to get my receptionist to call patients before appointments to remind them to come. Seems like a good, innovative solution, right? Wrong.
I haven’t actually gotten to the root of the issue. You need to really understand what is going on, lay out all the pieces, and then ask yourself - what’s the biggest driver of this problem? This is something called the Pareto method, where you essentially look for the 20% of reasons that are accounting for 80% of the problem.
By tweaking the most important players, you can fix most of the problem. You don’t need to fix everything, and you can let the surface-level stuff go.
In this example, it might look like this:

This shows me that forgetting appointments AND being too sick to come are big drivers of the issue. My plan to call the patient only fixes one of those. Also, even once you think you know what’s going on… you have to keep asking why. I cannot stress this enough. Don't stop asking why.
For this example, asking why would get you another diagram that looks like this:

Now we realize - calling the patient to remind them to come to the appointment won’t actually solve the issue, because they will just forget again! A better solution is to have the receptionist call the patient’s family member (who comes with them to the appointment) to remind them.
You have to get to the drivers of the problem, and solve those, or your innovation won’t work, and people won’t use it.
If you’re not sure, ask someone. Healthcare providers can usually tell you pretty quickly that something won’t work; but they might not be able to articulate why. They’ll say something vague, or be unimpressed by the idea. Take this as a sign that you’ve missed the mark. Try and ask more questions around the problem, and why they think it’s happening. Keep asking why until you get to the root.
This is also a great place to look to existing research. Implementation scientists often look at “barriers and facilitators” to different issues. You might find some ideas from doing a google search for those terms.
4. THEY DON’T HAVE THE BANDWIDTH AND/OR RESOURCES TO USE YOUR INNOVATION
There is a giant chasm of factors outside getting the problem and solution right that can impact your success. This is the frustrating piece for innovators, because even if you get #1-3 right, you still might be hitting a wall.
You can break down this chasm into internal and external circumstances.
Internal Circumstances
There are a number of “people factors” that impact whether an innovation will be used, with researchers finding many “sociological theories”. I’ve taken some of these theories, combined them with my real-world experience, and reframed them into 4 categories. If you want an example of a full scientific approach, check out the NASSS Framework, developed by researcher at the University of Oxford.
According to OG medicine your innovation might not be used if people lack enough bandwidth or resources in:
1. Emotional space
Burnout (lack of emotional space) is an important barrier to change and innovation. When healthcare workers are burned out, even something as small as switching the type of pen being used can feel like a huge task. I remember once crying all the way home from a 24-hour night on call because I dropped my favourite travel mug in the parking lot. This relatively minor event was too much when I was emotionally occupied with other stressors of healthcare.
In these situations, it doesn’t matter if your innovation is easy, efficient, and will make life better. There’s no emotional space to do something new. It’s survival mode.
Solution? … complicated. Check out my career & wellness posts for more insights, but overall, the system needs to change to reduce work-place stressors. Practically speaking, you’ll need to narrow your target users even further to those that aren’t burned out, or run some kind of wellness campaign leading up to the implementation of an innovation, if you sit in a powerful role in the healthcare system.

Burnout is emotional receptor overload - there’s no room left for anything new. Even if they have the physical time to incorporate a new innovation, they will feel like they don’t, because of the lack of emotional space. When all the receptors are full, additional messages cannot get through.
2. Emotional Triggers
The second internal circumstance that might be blocking your innovation is that you are inadvertently triggering certain emotions that make people naturally want to resist to protect themselves. This is an evolutionary response, and often people, including doctors, don’t realize that their emotions are impacting their actions. This can usually be broken down into:
a) Fear - if you or your innovation makes them feel nervous, exposed, excluded, insignificant, inferior, inadequate, worried, overwhelmed, or frightened.
b) Anger - if you or your innovation makes them feel betrayed, resentful, disrespected, ridiculed, indignant, jealous, annoyed, skeptical, and dismissive.
This ties in well with research that shows innovations get blocked when they threaten professional identities (i.e. threatening the doctor-patient relationship), invade on a professional’s scope of practice (i.e. tell them what to do), or are counter to their personal beliefs (i.e. they morally object to the concept of your innovation).
The solution is that you need to be really mindful of how your innovation, or your innovation pitch, is going to come off to your different user groups. Often it’s in the nuance of your phrasing and framing that you use.
For example, in the deprescribing startup, the value proposition to patients was access to safe, expert medication management. The value proposition to doctors was to help offload the time consuming process of deprescribing. Notice how we used “offload” (getting at #2), and didn’t imply that they couldn’t do the task themselves; just that we recognized how overworked they were, and we were there to help.
To summarize, be kind, assume the best in people, don’t insult anyone, and think about how your innovation might make them nervous or threaten their self-image.
3. Money
This is an obvious one. All innovations require someone to pay, and procurement in healthcare is complicated. The people using the innovation might not be the ones paying for it (i.e. the hospital might pay… but the patient uses it). Having a value proposition for each and every stakeholder (i.e. person who will touch your innovation in some way), is important.
Showing cost savings, or return-on-investment (ROI) is a helpful way to make your case, but this often requires you having people use the thing first so you can get the data to show the cost savings. This means you’ll need to start with the people who have the problem and the money to try it (we’re back to target market again).
4. Power
This last one is also obvious as soon as it’s down on paper. Someone might have your problem, love your solution, and want to use it, but they might not have the power to do so. A great example of this would be a medical resident - they’re young, usually more tech-savvy and improvement focused, and full of ideas and energy to change the system. They might seem like a great target for your innovation, but if the innovation requires them using it in places where they don’t have power - i.e. at the hospital (they do the work, but the attending physician has the ultimate power), then it’ll flop.
You’ve got to match your innovation to their circle of influence, or get both residents (who bring the energy) and attendings (who bring the power) on board.

The only things we can control 100% are our own thoughts, actions, and choices (and these are heavily influenced by things around us). We can influence some things - like what other people think, or what patients do - but we ultimately do not control the outcome.
External Circumstances
This has to do with the spaces, or context, within which the individuals move and work. Depending on their environment, individuals are more or less able to use your innovation.
This includes things like:
Organizational factors (slack resources, de-centralized decision making, strong leadership, risk-taking climate)
Conflicting value propositions (multiple stakeholders, opposition)
Financial constraints (budget, budgetary control, procurement)
Legal / regulation (professional standards, medicolegal responsibility)
I’m not going to go into each of these in detail because if you are an entrepreneur or healthcare worker trying to innovate, you won’t have much control over these things anyways. You’ll need to focus on finding the right organization to bring your innovation to (target market…again). If you run an organization in a management or policy-making role, then subscribe for future articles on how you can transform your organization into one that invites innovation, and check out this paper.

While the ultimate act of using an innovation rests with the individual healthcare worker, the decision to act exists in a layered reality, where the bigger picture impacts the individual’s ability to say “yes”. This can include but is not limited to hospital factors - leadership, resources, opposition; the healthcare system - provincial funding, local norms and practices - and the wider system - politics, legal and regulatory requirements, and media pressure.
To figure out whether a group (be it a clinic, hospital, healthcare network, or system) promotes innovation, I’ve come up with a highly not scientific but common-sense approach, that involves looking at the culture, which manifests in how people feel and act at work.
Is it a place where people are generally happy? Does it seem vibrant? Are cool things happening there? Or does it seem like an old stodgy castle where only tradition is followed, a house on fire with people running away, or a place where nothing ever changes and the same problems are argued about over and over.
To find out, don’t only talk to the leaders. Talk to the regular workers and middle-range people - the street-level bureaucrats, as they’re sometimes called. Follow your intuition when it comes to finding out what’s beneath the surface of an organization (if you don’t work there yourself already).

5. THEY DON’T TRUST YOUR INNOVATION
This is the final piece of the puzzle. You can have #1-4, but if people don’t trust you and your creation, they aren’t going to use it. Medicine is a highly regulated world because the stakes are high; patients lives are on the line. This creates tension between innovators, and in particular non-healthcare entrepreneurs, who are focused on “build fast and break things” and healthcare workers, who are focused on “be careful and don’t break things”.
That being said, physicians and other healthcare workers, like entrepreneurs, are actually quite comfortable with managing risk and uncertainty - we deal with it all the time. Doctors are constantly trying to recognize and reduce risk. We assess the probability of something (“what is the probability I’m missing a PE….) and mentally calculate an action (get the CTPE or don’t get the CTPE) to mitigate that risk. We use formal risk prediction tools (in this case, maybe the Well’s score, or a d-dimer), and combine that with clinical judgement, to decide what to do.
If you demonstrate the same risk reduction approach with your innovation, this will go a long way to developing trust with doctors. This includes things like having a medical director that oversees safety and risk, having research on safety data, consulting with the legal authority (CMPA) that protects doctors in Canada, and maybe even building a “risk chart” (which is actually required in the UK’s NHS digital healthcare technology regulatory process).
Doctors don’t expect the risk to be zero, but they expect you to have thought about it, and to have done something to address it, just like they do.

Risk management for clinical safety, used by the National Health Service in England to regulate digital healthcare technologies. For more info, click here.
The final and most powerful way to build trust is for a doctor to see another doctor they trust use your innovation. This is the power of social contagion, or network-spread, of an idea or innovation. It stems from the way that doctors were trained - by textbooks (medical school) but primarily by observation (residency and fellowship). We learned from watching others what was safe, what was normal, and what was considered good and effective care.
We continue to do the same when making decisions about new treatments or innovations. Asking “what are other people doing?” is a short-cut to vetting the solution ourselves. If others are using it and liking it, and I trust my colleagues, then it will probably be safe for me to use it too.
You can tap into this powerful network of trust by having both a peer opinion leader (i.e. someone who is similar to your intended user) and expert opinion leader (i.e. someone that your intended user looks up to for advice) use and promote your product. Pharmaceutical companies use this tactic all the time with great effect.
In a future blog, I’ll walk you through the other characteristics of social networks that facilitate the adoption of innovation in healthcare (my dissertation thesis at Oxford). Suffice is to say, multiple studies have shown that acceptance by professional staff might be the most important factor in whether a new technology will succeed.

Network spread of innovations is based on trust. People who trust other people copy each other as a surrogate for due-diligence themselves. If you can tap into the trust network, your idea will spread much more quickly and with much less resistance.
BONUS: YOUR INNOVATION NEEDS TO ADAPT
I’ve packed lots of key concepts and high-yield facts into this blog, but there is one more bonus point that is really important to understand. You need to be okay with your innovation being used differently by different people.
Take something as simple as a microwave - some of us use it to bake, others cook whole meals, and others use it simply to make popcorn. Something as simple and mundane as a microwave gets used differently in different households. Imagine how a complex innovation - like a new technology in healthcare - will be used differently by different healthcare workers, hospitals, and entire healthcare systems. The focus on sticking to the original design, or “fidelity” to the innovation, is an unhelpful fallacy that doesn’t actually happen in the real world.
You need to be okay with adapting to different users and different contexts if you want to succeed at scale.
PUTTING IT ALL TOGETHER
You now have an overview of the 5 main reasons why your innovation isn’t working in healthcare.
All 5 are essential to success, but #1-3 are a non-starter; if you don’t build a product that people want, you’re dead in the water (i.e. product/solution fit).
#4-5 touch on the wider context and continues to highlight the importance of finding the right target market. Ask yourself where are you planning to launch your innovation? Are they ready for change? Do the people have the innovation-spirit and resources? Or are they strapped, tired, and unable to innovate without significant infusion of resources?
Depending on who you are - a start-up entrepreneur with a lean VC fund - or a healthcare organization with a federal budget - you might be able to influence the readiness for change. The key is to know that this needs to be in place if you want to achieve success.
After all of that, the final silver bullet is gaining trust so that your innovation spreads through the social network of healthcare providers like wildfire. Lose trust, and things will quickly disintegrate in the close-knit and risk-weary community.

Good luck, and never lose your spark for innovation.
Olivia
Dr. Geen is an internist and geriatrician in Canada, working in a tertiary hospital serving over one million people. She also holds a masters in Translational Health Sciences from the University of Oxford, is widely published in over 10 academic journals, and advises digital healthcare startups on problem-solution fit and implementation. For more info, see About.
Influences:
Life experiences
Greenhalgh T, Wherton J, Papoutsi C, et al. Beyond adoption: a new framework for theorizing and evaluating nonadoption, abandonment, and challenges to the scale-up, spread, and sustainability of health and care technologies. J Med Internet Res, 2017;19(11):e367.
Conversations with Brandon Goode, CEO of Outro Health, and Dr. Richard Sztramko, co-founder of Arya Health.
List, J. Voltage Effect: how to make good ideas great and great ideas scale. 2022.